Atlantoaxial instability is an uncommon condition of dogs in which there is abnormal movement in the neck, between the atlas (first cervical vertebra) and axis (second vertebra). This instability allows abnormal bending between the two bones, which causes compression of the spinal cord. The severity of the injury to the spinal cord depends both on the amount of pressure, and the duration of the condition.
The atlantoaxial joint is normally stabilized by a projection off the axis called the dens, which fits into the atlas, as well as several ligaments between the two bones. There are two causes for the instability, trauma and birth abnormalities. Traumatic instability occurs after forceful flexion of the head, causing either fracture of the dens or other part of the axis, and/or tearing of the ligaments. This form of the instability can occur in any breed, at any age.
Certain birth defects can predispose this instability to occur with a very small amount of trauma (i.e. jumping off the couch, being jumped on by another dog). These abnormalities include a missing or malformed dens, or lack of normal attachments between the two vertebrae. An absent or smaller dens is the most common predisposing cause. This condition is seen mainly in small breed dogs, with Yorkshire terriers, Chihuahuas, Miniature or Toy Poodles, Pomeranians and Pekingese being the most frequently reported breeds. Dogs with congenital abnormalities usually show clinical signs at less than one year of age.
Symptoms can vary in severity. Onset of symptoms can be gradual, or can be very sudden. Neck pain is most common. This may be the only symptom; however, the degree of pain can be severe. Varying degrees of incoordination and weakness or paralysis from the neck down. With complete paralysis of all four limbs, paralysis of the diaphragm also occurs, and the animal is unable to breathe. Usually these dogs die very suddenly before they can receive medical attention. Some dogs may demonstrate intermittent collapse.
Diagnosis is based on signalment (breed and age), history, symptoms, and radiographs (x-rays).
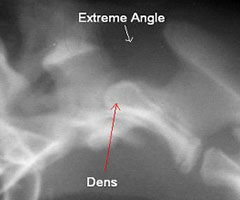
- Dorsal deviation or tipping of the axis can be seen on radiographs, with increased space between the atlas and axis (Figures 1 and 2).
- The dens may be small or absent, or visible fractures may be present.
- Certain views may be used to highlight these changes, such as gently flexing the neck, or taking radiographs from an angle or with an open mouth view. Extreme care must be taken to avoid excessive flexion forces.
- ACT scan can also be valuable to evaluate the vertebrae for other possible deformities.


Treatment can be conservative or surgical. Conservative management is more likely to be recommended when clinical signs are mild, or surgical treatment is not possible due to other medical conditions of your pet. Pets are managed with strict cage rest and a neck brace for several weeks. Steroids and pain medications may also be used, and your pet will need to be protected indefinitely from trauma. Complete recoveries have been reported, even for dogs with severe signs, but dogs can also either remain unchanged or deteriorate. With continued instability, there is a risk for suddenly dislocating the spine, with acute paralysis and death. Potential complications include:
- continued instability
- inadequate stabilization by the brace
- chronic spinal cord compression
- failure to heal fractures of the dens or body of the axis
- bandage sores and eye ulcers related to the splint/neck brace are frequently seen
Surgery is usually recommended over conservative treatment because of the possibility of recurrence and further spinal cord damage. Goals of surgery are to relieve pressure on the spinal cord, and permanently stabilize the joint. Pressure is usually relieved by reducing the vertebrae into a normal position. If the dens are malformed and is deviated towards the cord, occasionally it will need to be removed to relieve the compression. The joint can be stabilized with many different techniques. It can be stabilized from the top (dorsal) or from the bottom (ventral). Most surgeons will now use a ventral technique, as approaches from the dorsal side do not usually result in fusion of the two bones, and long-term stability relies on scar tissue and lasting strength of the implants.
Ventral techniques are currently preferred, as they allow removal of the joint cartilage to enable fusion, and placement of bone graft to stimulate this bony healing. This approach facilitates correct alignment and reduction, and removal of the dens if necessary. Ventral techniques include cross-pinning, trans-articular screws, a combination of pins or screws and bone cement, or bone plates (Figures 3a and 3b, 4a and 4b). The choice of repair is often dependent on surgeon preference, as well as size of the dog. Potential complications of surgery:
- Death due to sudden respiratory arrest with injury to the spinal cord during surgery.
- Breakdown of the repair with migration or breakage of the implants.
- Inadequate reduction or mal-alignment of the spine. Implants can be positioned incorrectly causing chronic pain or impingement of the spinal cord, and requiring removal. Improper positioning can be a problem due to the small amount of bone available to engage the pins or screws, and a very small target area in small dogs to avoid the spinal canal.



Strict rest is still required for 6–8 weeks after surgery. Neck braces for additional support may be used. Repeat radiographs (x-rays) will often be repeated in 4 and 8 weeks to assess the repair, and healing.
The prognosis for atlantoaxial instability depends on the degree of spinal cord trauma and neurological deficits already present. Good for dogs with mild clinical signs and guarded for dogs with paralysis, but significant recovery is possible, if decompressed and stabilized. Significantly greater success rates with surgery are seen in younger dogs (<2 years of age), dogs with more acute problems (<10 months of symptoms), and dogs with less severe neurological problems.
Premier Sponsors






