Due to the anatomical structure of the airway, the horse must breathe through its nostrils. The opening to the trachea sits at the back of the throat and is called the rima glottidis. Air is inhaled through the nostrils, passing through the rima glottidis, and into the trachea where it is transmitted to the lungs.
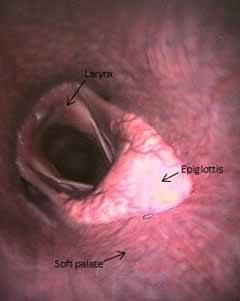
The soft palate is an extension of the hard palate that separates the oral cavity and the nasal cavity. The epiglottis is a triangular shaped piece of cartilage that flips upward to protect the rima glottidis during swallowing; preventing food from entering the trachea (Figure 1a). Importantly, the epiglottis sits on top of the soft palate to form a tight seal between the oral and nasal cavities. This allows the horse to breathe entirely through its nose and to achieve maximum airflow into the trachea and lungs
In a normal horse, the soft palate moves down, and the airway opens up to maximize the amount of room for air to pass into the lungs during intense exercise. Dorsal displacement of the soft palate (DDSP) describes the condition where the soft palate displaces upwards to sit on top of the epiglottis (Figure 1b). This causes the soft palate to obstruct the opening to the trachea and reduces the amount of airflow to the lungs.
DDSP is an expiratory disorder, meaning that increased expiratory pressures from exercise (canter, gallop) causes air to deviate underneath the soft palate so it sits on top of the epiglottis, reducing normal airflow in the trachea. This can lead to reduced ventilation and poor performance.
It is likely due to abnormal contraction of the muscles in the soft palate and throat, causing the soft palate to become flaccid. Less commonly, structural problems with the soft palate or epiglottis such as cysts, masses, or deformity of the epiglottic cartilage result in displacement of the soft palate. Additionally, some neurological conditions or conditions that damage the nerves that control swallowing and airway function can also result in DDSP.

DDSP often occurs intermittently, especially during intense periods of exercise, and can cause noisy breathing on exhalation that consists of gurgling or vibration. Some horses display billowing of the cheeks at high-speed exercise, coughing, and abrupt stopping during intense exercise (“choking down”/”hitting a wall”). When the horse swallows, the soft palate and epiglottis relationship usually returns to normal (epiglottis on top of the soft palate), and the horse can then proceed without difficulty, and the respiratory noise goes away.
The gold standard for diagnosis of intermittent DDSP is based on a history of poor performance with respiratory noise, and use of both endoscopic exam at rest and during exercise. Upper airway endoscopy must be utilized for the diagnosis of DDSP. Confirmation of this condition is best made with the use of overground endoscopy in which an endoscope is placed up the nostril to view the epiglottis and soft palate as the horse is exercised. If the soft palate displaces during exercise and is not immediately replaced, then a diagnosis of dorsal displacement of the soft palate can be made and steps aimed towards treatment can begin.
There are several causes of DDSP that need to be investigated even after upper airway endoscopy has confirmed displacement. Fitness is the first aspect that is addressed with this condition prior to any further intervention. Pharyngeal or upper respiratory tract inflammation on endoscopic examination should be treated with appropriate topical and oral anti-inflammatory agents. These causes must be evaluated and ruled out prior to recommending any surgical intervention for this condition.
Fitness is the first aspect that is addressed with this condition prior to any further intervention. The use of a figure-8 noseband to keep the horse from opening their mouth and bits such as the spoon or the Z bit are aimed at preventing the horse from playing with their tongue during exercise and thereby pushing the soft palate up into a displaced position. Any evidence of pharyngeal or upper respiratory tract inflammation on endoscopic examination should be treated with appropriate topical and oral anti-inflammatory agents.
Surgical Procedures for treatment of DDSP
Any treatment, whether surgical or medical, should aim at addressing the underlying cause of DDSP. The current recommended treatment for DDSP is the laryngeal tie-forward combined with a partial bilateral resection of the thyrohyoideous tendon/muscle.
The most common surgical procedures include the standard myectomy, the minimally invasive myectomy and the laryngeal tie forward.
- Standard myectomy is a partial resection of the sternohyoideus and sternothyroideus muscles, with or without omohyoideus resection. This procedure is performed to reduce caudal retraction of the larynx. Success rates vary from 58-70%.
- Minimally invasive myectomy is often a first line treatment. A portion of the muscle and the tendon of the sternothyroideus muscle are transected. This has the effect of bringing the epiglottis and soft palate into a more normal relationship so dorsal displacement of the soft palate no longer occurs. The success rate is 58-70%.
- Laryngeal advancement procedure (“Tie Forward”) involves permanently fixing the larynx forward by means of two permanent sutures placed between the thyroid cartilage and basihyoid bone. The distance between the epiglottis and the opening of the larynx is reduced thereby making it harder for the soft palate to displace above the epiglottis. The reported success rate is between 70-90%.
Following surgery, horses are typically maintained on antibiotics and anti-inflammatories for a short period of time, combined with rest for 2-4 weeks depending on the procedure. In the case of a Tie Forward, they are fed and watered at shoulder height to reduce stress on any sutures.
This condition can be frustrating to correct and may recur even after an initial period of success. This underlines the difficulty in knowing an exact cause in the majority of horses that are affected. After a thorough examination of the upper airway under various conditions, your veterinarian will be able to recommend the treatment option most likely to have the best impact on your horse.
Premier Sponsors






