Bone tumors can involve either the appendicular (limbs) or axial (spine, ribs, pelvis, scapula, and skull) skeleton. These tumors are classified as either primary (i.e., arise directly in bone) or secondary (i.e., spread from an adjacent site, such as multiple myeloma of the bone marrow or metastasize from a distant site, such as transitional cell carcinoma of the urinary bladder).
The four most common primary appendicular bone tumors found in companion animals are osteosarcoma, chondrosarcoma, fibrosarcoma, and hemangiosarcoma. In dogs, osteosarcoma is the most common primary bone tumor and accounts for over 85% of all bone tumors. Canine appendicular osteosarcoma is a highly aggressive disease and curative-intent treatment involves surgical resection of the tumor followed by chemotherapy to minimize the risk of tumor cells spreading (metastasizing) to other areas, particularly the lungs and other bones. While bone tumors are rarely found in cats, osteosarcoma is also the most common type of bone tumor and accounts for over 65% of cases. Feline osteosarcoma behaves less aggressively compared to canine osteosarcoma and curative-intent treatment can involve surgical resection without chemotherapy.
The majority of primary bone tumors, particularly osteosarcoma, arise spontaneously with no known or apparent cause. Scottish Deerhounds are genetically predisposed to developing osteosarcoma and this tumor also occurs frequently in other large breed dogs, particularly the Rottweiler. Large or giant, and particularly tall, dogs are at a greater risk for the development of osteosarcoma compared to the general dog population, although small dogs (less than 15 kg) can also be affected. There is a biphasic age distribution. Older dogs are most commonly affected (~10 years old); however, bone tumors can occur in young dogs as well (~2 years old).
In certain instances, tumors can occur at sites of previous bone damage. The types of bone damage, which have been linked with the development of primary bone tumors include fractures, orthopedic implants (used for fracture repair and total hip replacement), radiation therapy, and bone diseases (i.e., benign bone tumors, bone cysts, and infarcts [areas of bone without a blood supply]). It must be stressed, however, that the risk of developing a bone tumor after fracture, fracture repair, or total hip replacement is exceedingly rare and the vast majority of primary bone tumors develop spontaneously with no apparent predisposing cause.

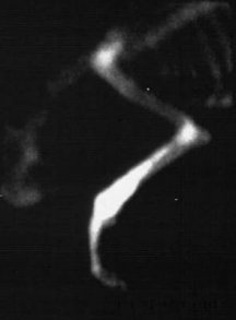
Lameness and swelling of the affected bone are the most common presenting complaints in cats and dogs with tumors of the appendicular skeleton. The onset and degree of lameness is variable: a slow, insidious onset of a mild to moderate weight-bearing lameness is more common, but an acute, non-weight-bearing lameness is possible if a fracture occurs where a tumor has weakened the bone (i.e., pathologic fracture) (Figure 1). It is rare for cats and dogs to display signs of systemic illness if the bone tumor has not overtly spread to other areas. Dogs with metastasis (spread the tumor) to the lungs may present with a diffuse swelling of all four limbs (hypertrophic osteopathy), generalized weakness, or respiratory (breathing) difficulties.
The clinical signs associated with primary bone tumors of the axial skeleton depend on the bone involved. In most cases, a swelling or mass is the first sign of a tumor, particularly in the skull, jaw, and ribs. Other signs may include:
- difficulty eating with jaw tumors
- neurologic signs with skull or vertebral tumors (e.g., seizures or wobbly gait)
- respiratory difficulties or lameness with rib tumors
Clinical signs associated with secondary bone tumors depend on the bone affected. However, differentiating primary bone tumors from secondary bone tumors can be difficult unless the primary tumor causes clinical signs (e.g., urinary difficulties in dogs with tumors of either the urinary bladder or prostate).

Diagnostic evaluation of a suspected tumor is called “staging”. Your primary-care veterinarian, sometimes with the help of specialists in oncology or surgery, may perform the following diagnostic tests to define what tumor type is present in the bone, where a tumor may have spread in the body, and to assess the overall health of your pet:
- physical and orthopedic examination
- blood tests (complete blood count and serum biochemistry)
- radiographs of the affected bone
- fine needle aspiration or biopsy of the bone
- chest radiographs or computed tomography (CT) scans
- whole body bone scan or radiographs (a radioactive marker is put in the bloodstream that can highlight bone tumors with a special imaging technology) or survey radiographs of other body parts
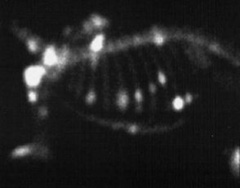
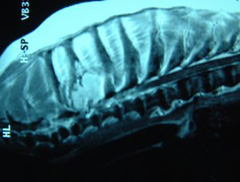
Physical examination is necessary to assess general health status and identify any other concomitant problems. Orthopedic examination is important to identify the affected bone, rule-out other causes of lameness (particularly cranial cruciate ligament rupture, hip dysplasia, and neurologic disease), and evaluate the potential for adapting to life on three legs if limb amputation is being considered. Blood tests are recommended to assess general health status, as many cats and dogs with primary bone tumors are older and may have other problems, which need to be considered when developing a treatment plan. Urinalysis may be added to assess kidney function. If a limb-sparing procedure is being considered, then radiographs, bone scans, and advanced imaging (i.e., CT or magnetic resonance imaging) of the limb should be considered to evaluate the extent of local tumor involvement and plan the limb-sparing surgery (Figures 2 and 3).
A biopsy (sampling of the suspected tumor itself) is important to determine the best treatment plan for your pet, because different tumor types respond differently to different treatments. The biopsy may indicate other causes of bony destruction. Biopsy is recommended if the presentation is not typical (e.g., small dog, middle aged, multiple lesions, lesions in the middle rather than the end of long bones, or systemic illness) or another disease process is suspected, such as a fungal bone infection, on the basis of presentation and either travel through or living in certain geographical regions.
For patients where destruction of the bone is extensive, a presurgical biopsy may not change the course to treatment and pathologic evaluation after amputation or limb sparing procedures may be elected. Fine needle aspiration may be used in some patients as a screening test for cancer, but often, a bone biopsy [where a core sample of the suspected tumor is obtained for review by a pathologist] is needed.
Appendicular osteosarcoma is a highly malignant and metastatic disease in dogs. The lungs and other bone are the two most common metastatic sites, occurring in approximately 10% of dogs at the time of diagnosis (but up to 90% of dogs during the course of the disease). Chest radiographs or CT scans are necessary for the evaluation of metastasis to the lungs. The incidence of bone metastasis, which often does not cause clinical signs, is approximately the same as lung metastasis but has a much greater impact on management options as there is a high risk of fracture through the metastatic lesion as a result of increased weight bearing after limb amputation. A whole-body bone scan is the most effective technique to evaluate for the presence of metastatic disease in another bone, although nuclear medicine facilities are not widely available (Figure 4). Whole-body radiographs are an alternative to bone scan but are more time consuming and costly, and metastases may be missed with radiographic evaluation because they are not as sensitive for picking up bone changes as a bone scan.
Advanced imaging, particularly CT scans, are recommended for many tumors of the axial skeleton as the cross-sectional and three-dimensional images provide better information for the ACVS board-certified veterinary surgeon to assess whether surgery is possible and, if so, the extent of surgery required for achieving a favorable outcome.
Following limb amputation or limb-sparing surgery, the tumor should be submitted to a veterinary pathology laboratory for assessment of tumor type and, if applicable, tumor grade (i.e., osteosarcoma and chondrosarcoma), whether the surgical margins are free of tumor cells (for limb-sparing surgery), and whether the tumor has spread to a regional lymph node.



Treatment for primary bone tumors of the appendicular skeleton is divided into palliative and curative-intent. Palliative treatment is intended to provide pain control and improve quality of life but not necessarily prolong life. In contrast, the aim of curative-intent treatment is to provide a good quality of life while controlling the local tumor and minimizing the risk of metastasis in an effort to cure the tumor. However, it must be stressed that cure for dogs with appendicular osteosarcoma is achieved in less than 25% of cases.
Palliative treatment options include pain-killing drugs, bisphosphonate therapy, radiation therapy, and surgery. Many drugs have pain-killing (analgesic) properties, but the degree of analgesia provided by these drugs can vary. Non-steroidal anti-inflammatory drugs are usually effective initially, although stronger analgesic drugs or drug combinations may be required as the tumor progresses. Radiation therapy can be used to reduce pain and inflammation and can be used in combination with pain-killing drugs and chemotherapy drugs. The bone tumor is irradiated using various protocols; the most common are either once weekly radiation for 3 to 4 weeks or once monthly radiation. Bisphosphonate therapy is used to induce the stoppage of bone degradation (osteoclastic activity), which can alleviate bone pain and diminishes pathologic bone turnover associated with osteosarcoma. Lastly, the affected limb can be amputated if the bone tumor is very painful or fractured. However, it should be noted that limb amputation without chemotherapy is palliative and does not prolong survival time.
For dogs with appendicular osteosarcoma, curative-intent treatment is aimed at treating the local bone tumor and minimizing the risk of metastatic disease. Limb amputation is recommended for treatment of the local bone tumor (Figures 5 and 6). If a tumor involves the hip or pelvis, a portion of the pelvis may be removed as well. The vast majority of dogs will adapt very well after limb amputation, even if arthritic in other joints, overweight, or a large dog breed. The adaptation period is approximately 4 weeks and is improved if pet owners have a positive attitude towards their dog and the treatment. Limb-sparing surgery preserves the anatomy and function of the affected limb and is a viable alternative to limb amputation (Figure 7). A number of different limb-salvage techniques are now available, but most are only amenable to the distal radius (bone adjacent to the carpus or wrist). Non-surgical limb-sparing techniques, such as stereotactic radiation, may be suitable for tumors in other locations. However, apart from preservation of limb function, there are no advantages of limb-sparing surgery compared to limb amputation. The decision to pursue limb-sparing surgery is usually a pet owner preference as there are few medical conditions, which would make limb amputation unfeasible. Furthermore, limb-sparing surgery is not widely available and the complication rate is relatively high. Following limb amputation or limb-sparing surgery, the tumor should be submitted to a veterinary pathology laboratory for assessment of tumor type and, if applicable, tumor grade (i.e., osteosarcoma and chondrosarcoma), whether the surgical margins are free of tumor cells (for limb-sparing surgery), and whether the tumor has spread to a regional lymph node.
Surgery, whether limb amputation or limb-sparing, is the only necessary treatment for cats with any type of primary bone tumor and dogs with primary bone tumors other than osteosarcoma or hemangiosarcoma. The majority of primary bone tumors in cats have a low potential to metastasize and hence do not require postoperative chemotherapy. In dogs, appendicular chondrosarcoma does have the potential to metastasize (less than 25%) but metastasis usually occurs late in the course of disease and chemotherapy has not been shown to affect the metastatic rate or improve survival time. Chemotherapy is recommended for dogs with appendicular osteosarcoma as survival time is significantly improved compared to surgery alone. Chemotherapy is usually started at suture removal (about 10 to 14 days after surgery). A number of different chemotherapy protocols have been used to treat dogs with osteosarcoma. The side effects and costs of these drugs vary and a consult with a medical oncologist is recommended to discuss these options.
The treatment for primary bone tumors of the axial skeleton is dependent on the size and location of the tumor. Surgery is the main treatment for axial bone tumors (i.e., mandibulectomy or maxillectomy for jaw tumors (see oral tumors), craniectomy for skull tumors, partial vertebrectomy for vertebral tumors (Figure 8), chest wall resection and reconstruction for rib tumors. Subtotal or total scapulectomy (removing part or all of the shoulder blade) may be performed for scapular tumors. Hemipelvectomy (removing a portion of the pelvis along with amputation) is indicated for many pelvic tumors. Analgesic drugs and radiation therapy can be used for palliation if surgery is not wanted or possible. Chemotherapy may be indicated following surgery however the metastatic potential for axial bone tumors, even osteosarcoma, is lower than the same tumor in the appendicular skeleton. Chemotherapy is recommended for dogs with osteosarcoma of the ribs, scapula, and pelvis because of a high metastatic rate and a biologic behavior similar to appendicular osteosarcoma. Chemotherapy should also be considered for mandibular osteosarcoma.
Limb amputation is considered the gold standard for the surgical treatment of primary bone tumors and the complication rate is very low. The most common complications, which occur in less than 5% of cases, are wound infection, wound breakdown, and accumulation of fluid underneath the surgical site (i.e., seroma formation). In contrast, the complication rate with limb-sparing surgery can be high. The most common complications are infection, implant failure, and local tumor recurrence. Implant failure is seen in 10% to 40% of dogs. Local recurrence of the tumor is diagnosed in 10% to 25% of dogs and this rate can be lowered with careful case selection and the use of locally-released chemotherapy implants (which are not widely available). Infection is the biggest problem with limb-sparing surgery and can be seen in 40-70% of dogs with these procedures. Antibiotics can control but rarely cure these infections. Interestingly enough, patients with limb-spare surgeries that develop a surgical site infection can have a significantly longer median survival time (480 days instead of 230 days). Other options for the treatment of limb-sparing-related infections include implantation of antibiotic-impregnated bone cement beads, isolated arterial perfusion of antibiotics, reconstructive surgery with skin and muscle flaps, and limb amputation.
The aim of chemotherapy is to kill the tumor while maintaining quality of life. The majority (more than 85%) of pets will progress through their chemotherapy protocol with no to minimal problems. However, 5% to 15% of dogs may require hospitalization to treat chemotherapy-associated problems, such as bone marrow suppression, infection, and dehydration from vomiting and diarrhea. The risk and severity of chemotherapy complications or side-effects are often dependent on the drug used and should be discussed with a medical oncologist.
For axial bone tumors, the complications are dependent on location of the tumor and the type and extent of surgery performed to remove the tumor. The type and risk of these complications should be discussed with your veterinary surgeon.
The majority of dogs are able to walk unassisted within 12 to 24 hours of limb amputation. Dogs should be encouraged to walk and exercise to improve the speed of recovery. The surgical wound should be checked twice daily for signs of infection or breakdown (called dehiscence). These signs include redness, swelling, watery to purulent discharge, and pain.
After limb-sparing surgery, the limb should be lightly bandaged and the bandages should be changed frequently for 2 to 3 weeks. Exercise is started immediately after surgery but should be restricted to leashed walks for the first 4 weeks. Exercise is important in preventing toe contracture and minimizing swelling of the foot and toes, both of which can occur as a consequence of excising certain muscles and blood vessels during surgery.
For dogs with appendicular osteosarcoma, the median survival time for following palliative treatment is 90 to 175 days, with 45-50% of dogs alive at 6 months and 15-20% alive at 12 months after diagnosis. However, median survival times of approximately 300 days have been reported following treatment with palliative radiation therapy and chemotherapy. In contrast, the median survival time following curative-intent treatment is 235 to 366 days, with up to 33-65% of dogs alive at 12 months and 16-28% alive at 2 years. Alkaline phosphatase is an enzyme analyzed in the preoperative blood tests, which has been shown to be associated with the duration of survival following surgery and chemotherapy. The median survival time for dogs with a normal alkaline phosphatase level is approximately 12.5 months compared to 5.5 months if alkaline phosphatase is increased at the time of diagnosis. Other factors that may influence prognosis in dogs with appendicular osteosarcoma include tumor size and location and histologic grade.
For dogs with appendicular chondrosarcoma, the survival time following limb amputation alone (i.e., no chemotherapy) ranges from a median survival time of 540 days to a mean survival time of 2618 days (median was not reached because less than 50% of dogs died as a result of their tumor). Grading of chondrosarcoma is important to determine prognosis because the median survival times for dogs with grade I, II and III chondrosarcomas are significantly different at 6 years, 2.7 years, and 0.9 years, respectively. Metastasis is reported in approximately 30% of dogs with chondrosarcoma, but this usually occurs late in the course of the disease and chemotherapy does not decrease the metastatic rate or improve survival time in dogs with chondrosarcoma.
Appendicular fibrosarcoma and hemangiosarcoma are rare and the prognosis is difficult to determine. However, metastasis is relatively common in dogs with hemangiosarcoma and, for this reason; survival times are generally poor with less than 10% of dogs alive at 12 months after limb amputation.
In contrast to dogs, cats with appendicular osteosarcoma have a low metastatic rate (less than 10%) and the median survival time following amputation alone is over 350 days (and up to 4 years).
The prognosis for axial bone tumors is dependent on tumor type and location. In general, osteosarcoma of the scapula and pelvis has a similar prognosis to appendicular osteosarcoma following either palliative or curative-intent treatment. The median survival times reported for osteosarcoma of the head (i.e., mandible, maxilla, and skull) are poor with most less than 12 months. The most common reason for this poor survival time is local recurrence of the tumor and not metastasis. However, the importance of aggressive surgical treatment is highlighted by the fact that most dogs are cured, with a median survival time greater than 1,500 days, if the tumor is completely resected.
Multilobular osteochondrosarcoma (multilobular tumor of bone) is a tumor of the axial skeleton and commonly affects the skull bones. The prognosis for dogs with multilobular osteochondrosarcoma depends on whether the tumor has been completely removed and on the histologic grade. Local tumor recurrence and metastasis are more common following incomplete tumor resection. The rate of local tumor recurrence is 30%, 47%, and 78% for grade I, II, and III multilobular osteochondrosarcoma, respectively. The metastatic rate of multilobular osteochondrosarcoma is also dependent on histologic grade, with metastasis, usually to the lungs, occurring in 30%, 60%, and 78% of grade I, II, and III tumors, respectively. The overall median survival time for dogs with multilobular osteochondrosarcoma is 669 to 797 days, with a median survival time greater than 897 days for dogs with grade I tumors, 520 days for dogs with grade II tumors, and 405 days for dogs with grade III tumors. Importantly, multilobular osteochondrosarcoma is a slow growing tumor and prolonged survival after diagnosis of metastatic disease is common (median, 239 days).
Rib osteosarcoma is an aggressive tumor. Metastasis is diagnosed at the time of death in 100% of dogs with osteosarcoma, 67% of dogs with hemangiosarcoma, and up to 100% of dogs with fibrosarcoma. Factors, which influence prognosis in dogs with rib tumors, include tumor type and completeness of surgical resection. Local recurrence of a rib tumor is over 5 times more likely if the rib tumor was not completely resected. The median survival time for dogs with rib osteosarcoma is 90 days with surgery alone and 240-290 days if surgery is combined with chemotherapy. In comparison, the median survival time for dogs with rib chondrosarcoma is 1,080 to greater than 3,750 days with surgery alone.
The prognosis for dogs with vertebral tumors is usually poor. Regardless of tumor type, the median survival time for malignant vertebral tumors is 135 days. Tumor type, tumor location, and postoperative treatment (i.e., chemotherapy or radiation therapy) do not improve survival time. However, using guidelines employed by human neurosurgeons, there are anecdotal reports of prolonged survival following aggressive surgical resection, with or without postoperative radiation therapy.
Premier Sponsors






